






Free · 5 minutes
Take the Perimenopause Self-Assessment.
Nine indicators, drawn from years of clinical work. If you recognise three or more, your body is asking you to look more closely.
Take the assessmentA short read for the woman who was told her IUD or her pill contains progesterone, who was told it would help, and who feels worse on it, with her sleep frayed, her mood low, her hair thinning, and no one explaining why.
Almost weekly in the clinic, a woman sits down and asks some version of the same question: she has been told that her IUD or pill contains “progesterone,” and that it should help, yet she feels worse on it. Her sleep is frayed, she is anxious, her mood is low, her hair has begun to thin, and her libido has fallen away.
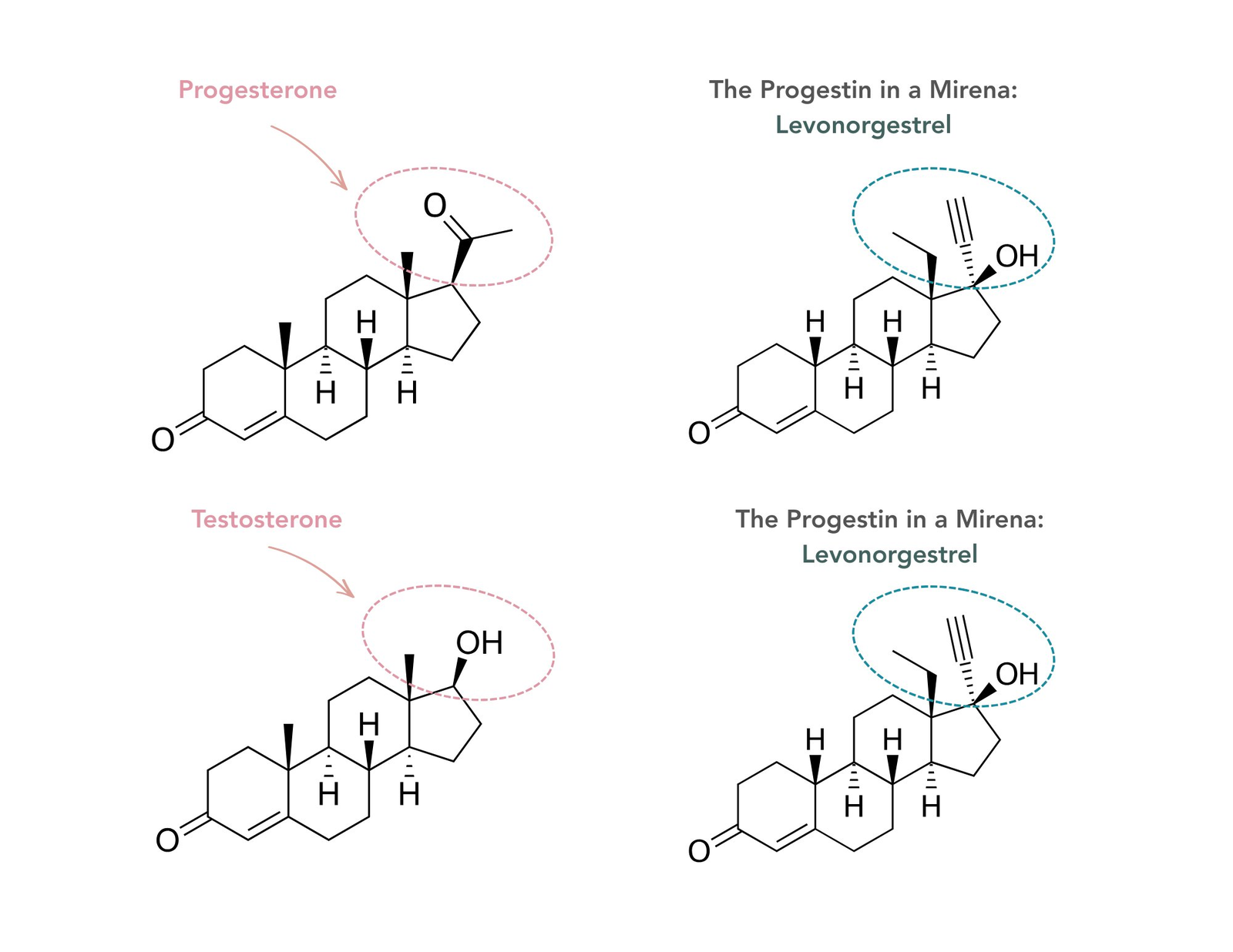
Bioidentical progesterone is structurally identical to the progesterone produced by the ovaries after ovulation. By contrast, synthetic progestins such as levonorgestrel, medroxyprogesterone acetate, norethisterone, and drospirenone are laboratory-made molecules designed to activate progesterone pathways for contraception or endometrial protection, but they differ in receptor activity and downstream effects. Pharmacology reviews emphasise that progestogens used in menopausal hormone therapy differ meaningfully in intracellular actions and clinical effects.
Some synthetic progestins, including levonorgestrel, are structurally related to testosterone, which helps explain why some women report androgenic side effects such as acne, oily skin, unwanted facial hair, or scalp hair thinning. Not all progestins behave the same way, however, and newer agents can be less androgenic or even anti-androgenic depending on the molecule.
The Women’s Health Initiative randomised trial of conjugated equine estrogens plus medroxyprogesterone acetate found an increased breast cancer risk, commonly described as about 24% to 26% higher than placebo. In contrast, the French E3N cohort found that estrogen combined with micronised progesterone was not associated with the same increase seen with several synthetic progestins, and a 2016 systematic review and meta-analysis reported lower breast cancer risk when estrogen was combined with progesterone rather than a synthetic progestin, with a relative risk of about 0.67.
For the levonorgestrel-releasing IUD specifically, recent Danish nationwide cohort data report a modestly increased breast cancer risk; one analysis found a hazard ratio of about 1.4 compared with non-users of hormonal contraception, with absolute risk remaining low at roughly 14 additional cases per 10,000 users. This should not be conflated with the WHI finding, because medroxyprogesterone acetate and levonorgestrel are different synthetic progestins with different pharmacology.
Micronised progesterone also has a separate body of evidence for symptoms. In a 2023 Phase III randomised trial in perimenopausal women, 300 mg oral micronised progesterone taken at bedtime did not significantly improve the trial’s primary vasomotor symptom score, but women did report significantly improved sleep quality and perceived reductions in night sweats, with no increase in depression. That makes the evidence for sleep more convincing than the evidence for hot flush relief in perimenopause.
The clinical pattern many women report on the Mirena can include mood changes, sleep disruption, acne, oily skin, scalp hair thinning, or reduced libido, although not every woman experiences these effects. Levonorgestrel is a synthetic progestin with androgenic potential, which helps explain why these symptoms can occur in susceptible users.
Breast cancer risk with levonorgestrel-releasing IUDs appears modestly increased in recent Danish registry data, but the absolute risk remains low. One important point of context is that the WHI result most often quoted in menopause discussions studied medroxyprogesterone acetate rather than levonorgestrel, so clinicians should avoid treating all progestins as a single risk category.
The differences between bioidentical progesterone and the synthetic progestins most commonly prescribed.
| Bioidentical progesteroneoral micronised progesterone | Synthetic progestinse.g. levonorgestrel (Mirena), norethisterone, medroxyprogesterone | |
|---|---|---|
| Sleep | Trials in peri and postmenopausal women suggest improved sleep quality and reduced nocturnal wakefulness, particularly at 300 mg taken at bedtime, although not all sleep outcomes were primary endpoints. | No good evidence that synthetic progestins improve sleep; some women report worse sleep or poorer overall tolerability. |
| Mood and anxiety | Often better tolerated from a mood perspective, and in the 2023 perimenopause trial micronised progesterone did not increase depression. | Some women experience mood swings, irritability, low mood, or anxiety, although effects vary by molecule and by individual. |
| Hot flushes and night sweats | Randomised data in perimenopause did not meet the primary vasomotor endpoint, but participants reported perceived improvements in night sweats and sleep, suggesting benefit for some women rather than a uniform effect. | No established role as a stand-alone treatment for perimenopausal vasomotor symptoms. |
| Breast cancer risk | Observational data suggest a more favourable breast safety profile than many synthetic progestins when combined with oestrogen, including the E3N cohort and the 2016 meta-analysis. | The Women's Health Initiative showed increased breast cancer risk with conjugated equine estrogens plus medroxyprogesterone acetate. Danish registry data suggest a modest increase with the Mirena, with low absolute risk. |
| Cardiovascular health | Available data suggest a relatively neutral cardiovascular profile compared with some older synthetic progestins, although robust outcome trials are limited. | Some synthetic progestins have been associated with less favourable lipid or blood-pressure effects and with higher cardiovascular event rates in certain oral combinations, though effects vary by molecule. |
| Metabolism and weight | Generally metabolically neutral in short-term studies, with no clear adverse effect on glucose or insulin; some women report less bloating. | Some synthetic progestins are associated with weight gain, fluid retention, bloating, or less favourable glucose control, though responses vary by preparation and individual. |
| Blood clot risk | Observational studies suggest transdermal oestrogen with micronised progesterone is not associated with the same venous thromboembolism risk seen with some oral estrogen-progestin regimens, but randomised outcome data are limited. | Oral oestrogen with certain synthetic progestins has been associated with higher venous thromboembolism risk than transdermal regimens and regimens using micronised progesterone. |
| Hair and skin | Not typically associated with androgenic side effects. | Testosterone-derived progestins such as the levonorgestrel in the Mirena may contribute to acne, oily skin, unwanted facial hair, or scalp hair thinning in susceptible women. |
| Overall tolerability | Often better tolerated in clinical practice and supported by a more favourable mechanistic and observational evidence base for several outcomes. | Side effects can be more prominent because many synthetic progestins interact differently with androgen, glucocorticoid, and mineralocorticoid pathways as well as progesterone receptors. |
| What it is best for | Endometrial protection in menopausal hormone therapy and, in some women, support for sleep and night-sweat symptoms. | Contraception and endometrial protection; symptom effects outside those indications depend on the specific progestin and should not be assumed to match progesterone. |
Observational and mechanistic evidence; effects vary by molecule and by individual. This supports an informed conversation with your prescriber, not a treatment decision on its own.
What this comes down to, beautiful, is which molecule is being prescribed and why. For most women navigating perimenopausal symptoms, bioidentical progesterone (oral micronised progesterone) tends to be the more favourable option: it is structurally identical to the progesterone your own body has been making since you were a teenager, the observational evidence on breast safety has been more reassuring than for many older synthetic progestins, and women generally tolerate it well.
Not all progestins behave the same way, and newer agents differ from older ones. The differences between molecules are real, and the right choice for you depends on what you are trying to achieve clinically.
This means asking the prescriber three things at your next appointment:
The answers should make sense to you. If they do not, that is a signal to ask further or to seek a second opinion.
The Vitality Clinic is where I work with women who are ready to have their hormones tested properly, their progesterone replaced bioidentically where appropriate, and their symptoms tracked clinically over time.
You can read more at workwith.thehollandclinic.com/the-vitality-clinic
I write about what women in my Vitality Clinic ask for, and what supports informed consent.
Or visit resources.thehollandclinic.com/more